|
|
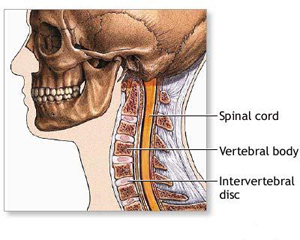
Neck pain may begin in any of the structures in the neck. These include muscles and nerves as well as spinal vertebrae and the cushioning disks in between. Neck pain may also come from regions near the neck, like the shoulder, jaw, head, and upper arms.
When your neck is sore, you may have difficulty moving it, especially to one side. Many people describe this as having a stiff neck. If neck pain involves nerves (for example, significant muscle spasm pinching on a nerve or a slipped disk pressing on a nerve), you may feel numbness, tingling, or weakness in your arm, hand, or elsewhere.
Causes
A common cause of neck pain is muscle strain or tension. Usually, everyday activities are to blame. Such activities include bending over a
desk for hours, having poor posture while watching TV or reading, placing your computer monitor too high or too low, sleeping in an uncomfortable position, or twisting and turning the neck in a jarring manner while exercising.
Traumatic accidents or falls can cause severe neck injuries like vertebral fractures, whiplash, blood vessel injury, and even paralysis.
Other causes include herniated disk, fibromyalgia (pain syndrome throughout the body), and arthritis. Meningitis, although much less common, can cause significant neck stiffness.
Home Care
For minor, common causes of neck pain: |
|
 |
Take acetaminophen or ibuprofen. |
|
Apply heat or ice to the painful area. One good method is to use ice for the first 48 - 72 hours, then use heat after that. Heat may be applied with hot showers, hot compresses, or a heating pad. Be careful not to fall asleep with a heating pad on. |
|
Perform slow range-of-motion exercises -- up-and-down, side-to-side, and from ear-to-ear -- to gently stretch the neck muscles. |
|
Gently massage the sore or painful areas. |
|
Try sleeping on a firm mattress without a pillow or with a special neck pillow. |
|
|
When to Contact a Medical Professional:
|
|
Seek immediate medical help if you have a fever and headache, and your neck is so stiff that you cannot touch your chin to your chest. This may be meningitis. |
|
Symptoms do not go away in 1 week with self care |
|
You have numbness, tingling, or weakness in your arm or hand |
|
Your neck pain was caused by a fall, blow, or injury -- if you cannot move your arm or hand. |
|
You have swollen glands or a lump in your neck |
|
Your pain does not go away with regular doses of over-the-counter pain medication |
|
You have difficulty swallowing or breathing along with the neck pain |
|
|
|
The doctor will perform a physical examination and ask detailed questions about your neck pain, such as: |
|
|
Is your pain in the front, back, or side of your neck? |
|
Are both sides of your neck affected equally? |
|
When did the pain first develop? |
|
Is it painful all the time or does pain come and go? |
|
Can you touch your chin to your chest? |
|
What makes your neck feel worse? What makes your neck feel better? |
|
Do you have neck weakness or neck stiffness? |
|
Do you have any accompanying symptoms like numbness, tingling, or weakness in your arm or hand? |
|
Do you have swollen glands or a lump in your neck? |
|
|
| The following diagnostic tests may be performed: |
|
X-rays of the neck |
|
CT scan of the neck or head |
|
Blood tests such as a complete blood count or a thyroid test |
|
A spinal tap for a cerebrospinal fluid analysis if meningitis is suspected |
|
MRI of the neck |
|
Prevention |
|
Use relaxation techniques and regular exercise to prevent unwanted stress and tension to the neck muscles. |
|
Learn stretching exercises for your neck and upper body. Stretch every day, especially before and after exercise. A physical therapist can help. |
|
If you tend to get neck pain from exercise, apply ice to your neck after physical activity. |
|
Use good posture, especially if you sit at a desk all day. Keep your back supported. Adjust your computer monitor to eye level. This prevents you from continually looking up or down. |
|
If you work at a computer, stretch your neck every hour or so. |
|
Use a headset when on the telephone, especially if answering or using the phone is a main part of your job. |
|
When reading or typing from documents at your desk, place them in a holder at eye level. |
|
Evaluate your sleeping conditions. Make sure your pillow is properly and comfortably supporting your head and neck. You may need a special neck pillow. Make sure your mattress is firm enough. |
|
Use seat belts and bike helmets to prevent injuries. |
| |
|
|
|
|
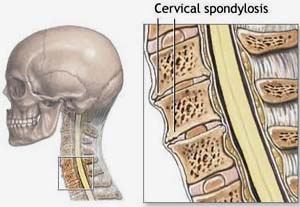
Cervical spondylosis is caused by degenerative changes in the bones and intervertebral disks of the neck. Cervical spondylosis is primarily due to aging. The condition usually first starts after the age of 40 and continues to progress as you age. Men tend to develop cervical spondylosis at an earlier age than women. The condition often leads to myelopathy. Cervical spondylosis is the most common condition of the neck that can affect the spinal cord.
What Happens
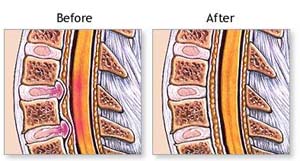
With age, osteophytes, or bone spurs, form on vertebral bodies. It's the body’s way of attempting to increase the surface area and stabilize the hypermobile vertebral joint. Generally not successful in this mission, the bone spurs can become painful as they put pressure on spinal nerves, and in some cases the spinal cord. This pressure often produces weakness, numbness and/or incontinence of either the bowels or the bladder.
Risk Factors for Cervical Spondylosis
Cervical spondylosis is more common in people who have had neck injuries. Such trauma might include work and recreational-related stress, for example:
|
|
|
carrying axial loads on your head |
|
professional dancing |
|
professional gymnastics |
|
Certain congential, genetic and acquired risk factors for cervical spondylosis have been identified by researchers: |
|
|
The condition may run in families. |
|
A congenitally narrow spinal canal increases the risk of developing cervical spondylosis with myelopathy. Spinal canals also narrow as a result of the age-related changes of thickening of spinal ligaments and bone. This type of narrowing has the same effect as congenital narrowing. |
|
Several varieties of excessive segmental motion such as atlantotaxial instability, often present in persons with Down syndrome, cerebral palsy and rheumatoid arthritis, are known risk factors. |
|
Smoking contributes to degenerative disk disease, and is therefore a risk factor. |
|
History of trauma predispose one to cervical spondylosis. |
|
|
Neck and shoulder pain are the most common symptoms. Types of neck and shoulder pain include: |
|
stiff neck, most often one of the very first signs. Neck stiffness tends to grow progressively worse over time. |
|
Radiating pain to the bottom of the skull and/or to the shoulder and down the arm. This radiating pain may seem like a stabbing or a burning, or it might present itself as a dull ache. |
|
Along with pain, cervical spondylosis can be accompanied by parathesias and muscle weakness in the neck, shoulders, arms and hands, and a syndrome called “numb, clumsy hands”. In cases of cervical spondylosis with myelopathy, the legs may be affected, leading to an interruption of stability while walking. Loss of balance might also occur. When myelopathy is present, incontinence may become a problem. Muscle wasting also accompanies cervical spondylosis with myelopathy.
Unfortunately, cervical spondylosis is a condition that gradually gets worse. In very advanced cases of this condition, often mobility can only be achieved with a cane or walker.
Seeking Professional Help for Cervical Spondylosis
It is time to seek medical help for cervical spondylosis when: |
|
your over-the-counter medicine does not keep your pain at bay. |
|
your pain continues to worsen |
|
your arms and/or legs develop numbness |
|
you experience weakness |
|
you experience bowel or bladder incontinence |
|
|
Diagnosing Cervical Spondylosis with Flexibility Tests and X-Rays
Doctors diagnose cervical spondylosis by means of neck flexibility tests and imaging techniques.
Neck flexibility tests are used to identify any instability that may be present in the neck. The tests include: tilting head to either side & rotating head to either side.
Imaging diagnostics of the neck are performed to see bone spurs and other anatomical changes associated with the condition. The imaging methods used include x-rays, which are an inexpensive way to see the narrowing of the canal and disk space, and the presence of arthritis in people who have the symptoms of cervical spondylosis. X-rays also give visual information about the integrity of the cervical curve.
Diagnosing Cervical Spondylosis with MRIs, CT Scans and other Tests
Other imaging diagnostics include:
|
|
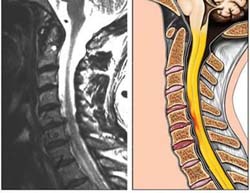
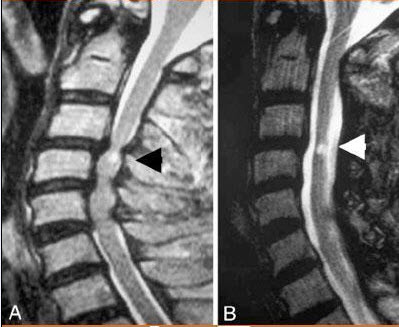
MRIs – Particularly useful for viewing the condition of the spinal nerves and the spinal cord. MRIs take pictures from many angles. |
|
CT scans provide good views of the bones, especially where they encroach on nervous tissue due to their reshaping over time. |
|
Myelogram – this imaging technique enhances the visibility of x-rays. They are expecially good for seeing problems located at nerve roots. |
|
In cases of Down syndrome and other conditions associated with atlantotaxial instability, visual images of the cervical spine in flexion and in extension might be taken to assist the doctor in determining the direction of treatment.
Sometimes electrical activity of the nerves and/or spinal cord is measured (by means of somatosensory evoked potentials or motor evoked potentials) to diagnose radiculopathy or myelopathy. Such tests may help to determine the presence of myelopathy, as well as the length of time the cervical spondylosis has been present in the spine, and if it is the cause of any found nerve root problem.
|
|
Treatment of Cervical Spondylosis and Arthritis of the Neck
Treatment of cervical spondylosis should reduce pain and irritation to spinal cord and nerves, while also improving activities of daily living. Treatment modalities may include:
The long-term prognosis in cervical spondylotic myelopathy is less clear. Some patients experience a progressive decline, while most have long periods of stability of symptoms with intermittent exacerbations.
Medical treatments for cervical spondylosis include neck immobilization, pharmacologic treatments, lifestyle modifications, and physical modalities (eg, traction, manipulation, exercises).
|
|
Neck immobilization (with a soft collar, Philadelphia collar, rigid orthoses, Minerva jacket, or a molded cervical pillow for support) is a common, nonoperative treatment for neck pain and/or suboccipital pain syndromes caused by spondylosis and cervical radiculopathy. Despite widespread use, soft collars are largely believed to work by placebo effect because they do not appreciably limit motion of the cervical spine. The collar should be worn as long as possible during the day. However, patient comfort is key. As symptoms improve, the collar can be worn only during strenuous activity. Eventually, it can be discontinued. |
|
Pharmacologic treatment includes several options. |
|
Myelogram – this imaging technique enhances the visibility of x-rays. They are expecially good for seeing problems located at nerve roots.
NSAIDs are the mainstay of pharmacologic treatment. They are effective in reducing the biologic effects of inflammation and pain.
Muscle relaxants such as carisoprodol and cyclobenzaprine may also be beneficial in patients with a spasm in the neck muscles (which can be related to spondylotic changes).
Opioids could be considered in patients who have moderate-to-severe pain due to significant structural spondylosis, whose who are poor surgical candidates, and those who have failed nonopioid agents..
|
|
Lifestyle modifications (eg, neck schools, instruction in body mechanics, relaxation techniques, postural awareness, ergonomics and/or workplace modifications) may alleviate symptoms.
Instruction in body mechanics focuses on low-load concepts. These include avoiding forward bending and rotation of the neck, avoiding prolonged extension of the neck, avoiding prolonged sitting or standing, and selecting the proper chair.
|
|
Physical modalities are among the oldest treatments used for spine-related disorders.
Cervical mechanical traction, commonly used for cervical radiculopathy, in addition to cervical joint distraction, may loosen adhesions within the dural sleeves, reduce compression and irritation of discs
Manipulation, most commonly practiced by chiropractors and osteopathic physicians, was described as early as 4000 years ago. It remains a popular treatment for back pain.
Techniques vary and include low-velocity, high-amplitude manipulation; high-velocity, low-amplitude manipulation (eg, thrusting or impulse manipulation); and nonthrusting maneuvers.
|
|
Exercises designed for cervical pain include isometric neck strengthening routines, neck and shoulder stretching and flexibility exercises, back strengthening exercises, and aerobic exercises. |
|
Other commonly used modalities for pain include heat, cold, acupuncture, massage, trigger-point injection, transcutaneous electrical nerve stimulation, and low-power cold laser. |
|
Surgery for Cervical Spondylosis
Surgical care for cervical spondylosis involves anatomic correction of the degenerative pathologic entities that compress a nerve root or the spinal cord.
Indications for surgery include intractable pain, progressive neurologic deficits, and documented compression of nerve roots or of the spinal cord that leads to progressive symptoms. Several approaches to the cervical spine have been proposed. The most common surgical options include: |
|
Frontal approach (anterior): The Surgeon makes an incision in the front of your neck and moves aside the windpipe (trachea) and swallowing tube (esophagus) to expose the cervical spine. Your surgeon can then remove a herniated disk or bone spurs, depending on the underlying problem. Sometimes, with disk removal, your surgeon will fill the gap with a graft of bone or other implant.
With the anterior approach, surgeon can relieve pressure on your spinal cord from bone or from multiple disk protrusions by removing two disks and the bone between them (corpectomy). Then, to support your head and neck, Surgeon reconstructs the area with bone from your body or a bone bank or with an implant made of metal combined with bone.
|
|
Back approach (posterior) : Surgeon may opt to remove or rearrange bone from the back of your neck, especially if several portions of the channel that houses the cord have narrowed. The operation, called a laminectomy, removes the back part of the bone over the spinal canal through an incision in the back of your neck. Laminoplasty, an alternative to laminectomy, involves cutting and moving pieces of vertebrae to make more room for the spinal cord. |
|
The primary goal of surgery for cervical spondylotic myelopathy is decompression of the spinal cord. The purpose of surgery for spinal stenosis is to relieve pressure on the spinal cord and/or nerves, and also to provide spinal stability.The most common surgery performed for spinal stenosis cases is the decompressive laminectomy. In this procedure, the lamina and spinous process of the vertebra are removed |
|
|



.png "Pinterest")